
Sacral Stage 4 Pressure Injury
Patient Overview
The patient is a 67-year-old male with a complex medical history, including a non-ST elevation myocardial infarction followed by a prolonged hospitalization and inpatient rehabilitation. His history is further notable for dysphagia with PEG-tube dependence on 2.0 CAL HN formula, chronic oxygen use at 1.5–2 L/min via nasal cannula, prior tracheostomy, atrial fibrillation, ventricular septal defect, benign prostatic hyperplasia, anemia, hyperlipidemia, gastroesophageal reflux disease, insomnia, constipation, acute kidney failure, hypotension, and a prior acute myocardial infarction. He is homebound, lives with his wife, is a former smoker, and denies alcohol or drug use. He has no known drug allergies.
His current medications include amiodarone, tramadol, aspirin, atorvastatin, ergocalciferol 50,000 units weekly, midodrine, pantoprazole, tamsulosin, vitamin C, and Juven taken twice daily.
Presentation
The patient presents with a chronic, non‑healing Stage 4 sacral pressure injury that developed during his hospitalization. The wound onset was January 2025, making it approximately four months old at the time of evaluation. His reported pain level at the time of assessment was 8 out of 10.
Failed Standard of Care
Hydrofera blue with dressing changes three times weekly, reinforcement of repositioning every two hours, and evaluation of mobility aids to reduce prolonged pressure. Systemic and nutritional optimization was addressed by increasing protein intake to 1.5–2.0 g/kg/day, adding Vitamin C 500 mg BID, Zinc 220 mg daily, and a daily multivitamin, and continuing Juven twice daily. Anemia management was initiated with ferrous sulfate 325 mg PO daily. Pain management with Tramadol.
Treatments
The wound bed and surrounding skin were cleansed using wound cleanser and sterile 4×4 gauze, followed by a final rinse with sterile saline. DermaBind FM was applied directly to the wound bed and trimmed to fit the wound contours, ensuring full and uniform contact. A sterile contact layer was placed over the graft, followed by gauze and a sacral foam dressing to secure it in place. The patient was followed primarily on a weekly schedule, with occasional variability in visit timing, resulting in an overall average interval of approximately
8.7 days.
Findings
The wound initially measured 35.75 cm² at the time of DermaBind application #1. After application #8, the patient was admitted to the hospital for an unrelated condition, during which standard of care was used until the follow-up visit on 7/29/25, when treatment proceeded with application #9. At this visit, the wound had increased to approximately 6 cm².
At the tenth application on 8/5/25, the wound had contracted to approximately 2 cm², and the final graft was applied at this visit. A follow-up occurred a little over two weeks later, during a period when the patient was relocating homes. During this transition, the provider noted some difficulty reaching and coordinating with the patient, reflecting common real-world factors that can influence continuity of care. Despite these logistical challenges, a visit was conducted on 8/21/25 and the wound was observed to have achieved 100% re-epithelialization, and the patient reported a pain level of 0/10, indicating a highly favorable clinical response.
| Date | Graft # | Length (cm) | Width (cm) | Depth (cm) | Surface Area (cm²) | Volume (cm³) |
|---|---|---|---|---|---|---|
| 5/12/2025 | Pre Graft | 6.5 | 5.5 | 3 | 35.75 | 107.25 |
| 5/17/2025 | DermaBind FM Application #1 | 6.5 | 5.5 | 3 | 35.75 | 107.25 |
| 5/24/2025 | DermaBind FM Application #2 | 4.5 | 5.5 | 3 | 24.75 | 74.25 |
| 5/31/2025 | DermaBind FM Application #3 | 4.5 | 4 | 2 | 18 | 36 |
| 6/9/2025 | DermaBind FM Application #4 | 4.5 | 3 | 1.7 | 13.5 | 22.95 |
| 6/16/2025 | DermaBind FM Application #5 | 3.5 | 2.5 | 1 | 8.75 | 8.75 |
| 6/23/2025 | DermaBind FM Application #6 | 3 | 2 | 1 | 6 | 6 |
| 6/30/2025 | DermaBind FM Application #7 | 3 | 1.5 | 1 | 4.5 | 4.5 |
| 7/8/2025 | DermaBind FM Application #8 | 3 | 1.5 | 1 | 4.5 | 4.5 |
| 7/29/2025 | DermaBind FM Application #9 | 3 | 2 | 1 | 6 | 6 |
| 8/5/2025 | DermaBind FM Application #10 | 2 | 1 | 1 | 2 | 2 |
| 8/21/2025 | 100% Re epithelialization | 0 | 0 | 0 | 0 | 0 |

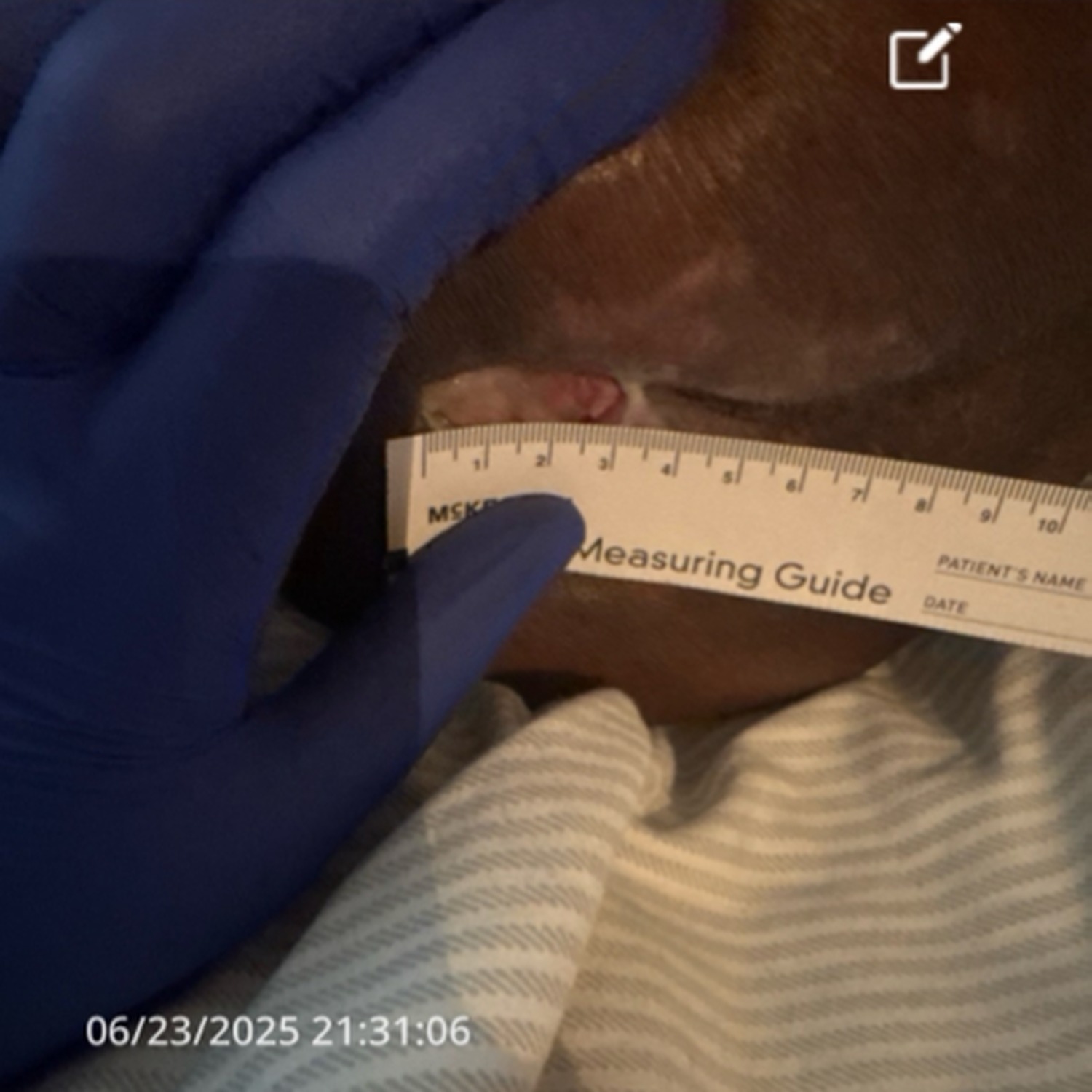
Before & After Wound Images











Ethical approval and patient consent
Institutional Review Board approval was not required for this one patient case as patient had already been treated by their provider with DermaBind based on medical necessity and failed conservative treatment. Patient consent was obtained by their provider for the use and release of deidentified data, and publication of photographs/images.
References
Mendivil, J., McMahon, A. E., Ojelade, O. T., Hobson, K., Marballie, M., Alvarez, S., Adu‑Aboagye, V., Chiamba, G., Gowdie, D., Landrum, W. E. II, Alzindani, A., Yazdani, H., Petty, G., Simard, M.‑C., Schmid, D., & Meadors, J. (2025). Clinical use of DermaBind TL/FM as a wound covering for hard‑to‑heal wounds of various aetiologies: A case series. Journal of Wound Care, 34(11). https://doi.org/10.12968/jowc.2025.0448
Provider Information
Provider Name: Vivian Adu-Aboagye APRN,FNP-C